Interventional Endoscopy Services:
- What is Upper GI endoscopy or EGD?
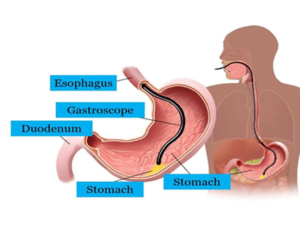
An upper GI endoscopy or EGD (esophagogastroduodenoscopy) is a procedure to diagnose and treat problems in your upper gastrointestinal (GI) tract. The upper GI tract includes your food pipe (esophagus), stomach, and the first part of your small intestine (the duodenum).
How does the procedure work?
You should not eat or drink 8hours before the procedure. You will be conscious but either sedated or the nurse will give you a local numbing (anesthetic) solution. It is important that you stay calm and breathe from the nose during the procedure. The procedure will last around 5-15 minutes.
What can be done with EGD?
- Bleeding control from upper GI tract.
- Removal of growths (polyps).
- Open (dilate) narrowed areas (strictures).
- Esophageal and Enteral stenting.
- Remove things that may be stuck in upper GI tract.
- Insert a tube used for tube feeding (a percutaneous gastrostomy tube) into the stomach (PEG tube).
- Banding of abnormal veins in your esophagus (Esophageal varices)
- Management of Tumors, either cancerous (malignant) or non cancerous (benign)
- Damage caused by swallowing very harmful (caustic) substances, such as household detergents and chemicals.
- Botox injections for Achalasia
- Balloon dilatation for Achalasia
- Gastric balloons for obesity and weight management.
Small bowel endoscopy is the procedure to look deep into your small intestine. It can be done with Enteroscopy or Capsule endoscopy.
Enteroscopy
What is enteroscopy?
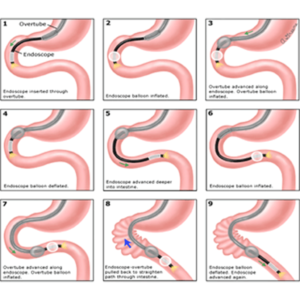
Enteroscopy typically refers to a more extensive endoscopic examination of the small intestine, extending into the jejunum and/or ileum. It includes several types of procedures that allow a physician to look further into the small bowel (which is up to 20 feet long). Enteroscopy is primarily used to find the source of intestinal bleeding, but can also be used to find lesions and determine causes for nutritional malabsorption.
How does the procedure work?
A physician may use a longer conventional endoscope, a double-balloon endoscope. You should not eat or drink 8hours before the procedure. You will be conscious but sedated. The procedure will take around one hour.
What can be done?
- Treatment of small bowel bleeding sources (Angiodysplasia).
- Management of small bowel polyps.
- Management of small bowel narrowing (strictures).
Capsule Endoscopy
What is capsule endoscopy?
Capsule endoscopy is a procedure that involves swallowing a small capsule, which is the size of a large vitamin pill. The capsule contains a tiny wireless camera that takes thousands of pictures as it passes through the small intestine. Images are transmitted to a recording device worn on a belt around your waist.
After ingestion of the capsule, you should come back to your doctor, who will remove the recorder. You can safely flush the capsule.
What is the benefit of capsule endoscopy?
It is a minimally invasive procedure. It can benefit patients suffering from
- Chronic abdominal pain
- Unexplained weight loss
- Unexplained blood loss
It can also use to diagnose disease deep into your small intestine.
- Crohn’s Disease
- Gastrointestinal Bleeding
- Celiac Disease.
- Ulcerative Colitis.
- Tumors
- What is Lower GI endoscopy?
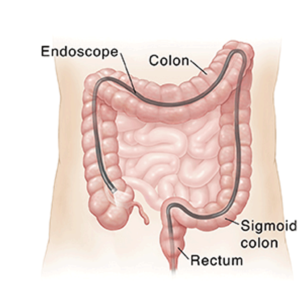
Lower GI endoscopy allows your doctor to view your lower gastrointestinal (GI) tract. Your entire colon and rectum can be examined (colonoscopy). Or just the rectum and sigmoid colon can be examined (sigmoidoscopy).
How does the procedure work?
A nurse will educate and give you a leaflet for the preparation of the procedure. You will be conscious but sedated during the procedure. Colonoscopy can take 30 minutes or longer. Sigmoidoscopy often takes about 20 minutes. The length of the procedure depends on how clean your intestines are, the reason for the procedure, and what treatments must be done.
What can be done with Lower GI endoscopy?
- Endoscopic mucosal resection (EMR) of abnormal growth (polypectomy) or abnormal looking mucosa.
- Management of bowel narrowing (strictures).
- Colonic stent placements for benign and malignant disease.
- Band abnormal veins in your rectum (Hemorrhoids)
- Management of colonic Tumors, either cancerous (malignant) or non-cancerous (benign).
- What is an EUS?
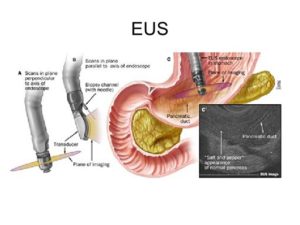
Endoscopic ultrasound (EUS) is a minimally invasive procedure to assess digestive tract (gastrointestinal) diseases. A special endoscope uses high-frequency sound waves to produce detailed images of the lining and walls of your digestive tract and nearby organs such as the pancreas, liver, and lymph nodes. EUS allows your doctor to sample (biopsy) fluid and tissue from your abdomen for analysis.
How does the procedure work?
You should not eat or drink 8hours before the procedure. You will be conscious but sedated. The procedure lasts for 30 to 60min.
What can be done with EUS?
- EUS guided gall bladder drainage.
- EUS guided biliary drainage.
- EUS guided Gastroenterostomy.
- Staging EUS for Biliary and Pancreatic tumors.
- Staging EUS for Esophageal and Gastric tumors.
- Celiac nerve block.
- Pancreatic cyst drainage with lumen opposing metal or plastic stent placement.
- EUS guided fine needle aspiration (FNA) & fine needle biopsy (FNB) of Pancreatic, Gastric, Biliary, Mediastinal and abdominal lymph node malignancies.
- What is ERCP?
Endoscopic retrograde cholangiopancreatography, or ERCP, is a specialized technique used to study the bile ducts, pancreatic duct and gallbladder. Ducts are drainage routes; the drainage channels from the liver are called bile or biliary ducts and the pancreatic duct is the drainage channel from the pancreas. An ERCP is performed primarily to correct a problem in the bile ducts or pancreatic duct.
How does the procedure work?
ERCP is done under general anesthesia. It is done with specialized side view scope and with the help of radiological images your doctor will assess and treat problems in biliary or pancreatic ducts. The procedure lasts for 30 to 60min.
How ERCP will help?
- Endoscopic evaluation and management of Gall bladder & Pancreatic cancers, and Cholangiocarcinoma.
- Management of Bile duct stones and strictures.
- Metal and plastic stenting of bile ducts.
- Biopsy and brushing of biliary cancers and strictures.
- Management of Pancreatic duct stones, and strictures.
- Sphincter of Oddi dysfunction.

THE TEAM

Dr. Usman Iqbal Aujla
Chairman Gastroenterology / Hepatology
Consultant Gastroenterologist, Hepatologist and Interventional Endoscopist